Cardiovascular Tutorial
A Picture is Worth...
***************************
This system consists of the heart and the blood vessels. Vessels that carry blood away from the heart are called arteries and those that carry blood toward the heart are called veins. Capillaries, short, thin-walled vessels, lie within the various organs and connect arteries to veins.
Key
The model is based on cause-and-effect relationships. The 'cause' is at the start of an arrow and the 'effect' at its end. If both the cause and the effect react in the same manner (both increase or both decrease) the relationship is direct. If they react in opposite manners (one increases and the other decreases) the relationship is inverse.
Direct and inverse cause-and-effect relationships are represented as follows:
- Nerves
- Direct: a solid line with bar
- Inverse: a dashed line with bar
- Physical
- Direct: a solid line with arrowhead
- Inverse: a dashed line with arrowhead
Design of the Model
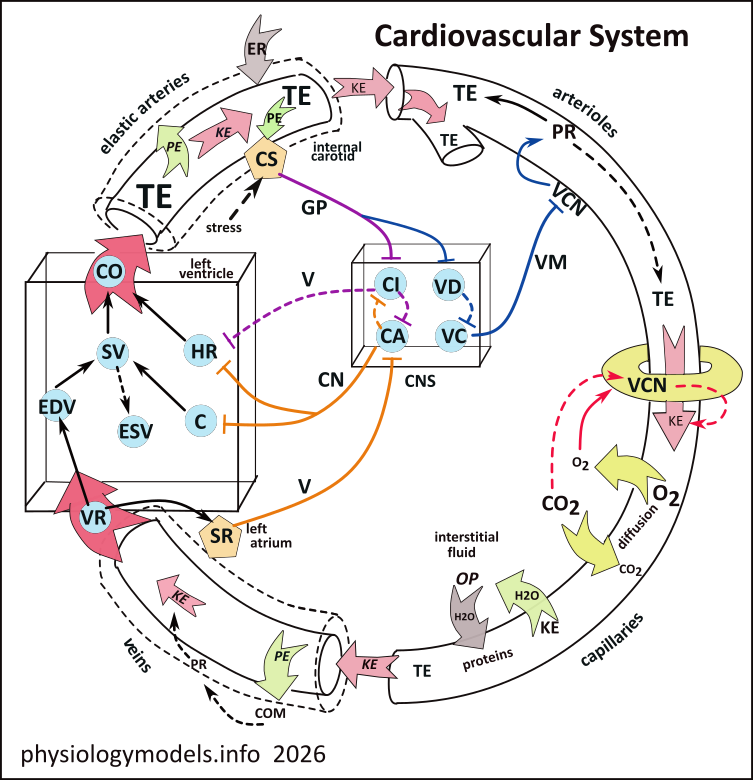
The cardiovascular system consists of the heart and blood vessels. Vessels leaving an organ are called arteries which give rise to smaller vessels called arterioles. These give rise to capillaries that recombine to form veins which return blood to the heart.
The central nervous system (CNS) has two cardiac centers (CA and CI) that control heart rate and contractility, the two vascular centers (VC and VD) control the diameter of arterioles.
The block arrow at the top of the heart box represents blood flowing from the heart into the arterial system; CO is cardiac output, the volume of blood leaving the heart each minute. The block arrow (bottom of heart box) represents blood flowing from the venous system into the heart; VR is venous return, the volume of blood returning to the heart each minute.
The small, red block arrows within the vessels represent the flow of blood due to its kinetic energy (KE). The donut structure at the beginning of the capillary represents precapillary sphincters that constrict and relax to regulate the flow of blood into capillary beds.
***************************
Blood Flow
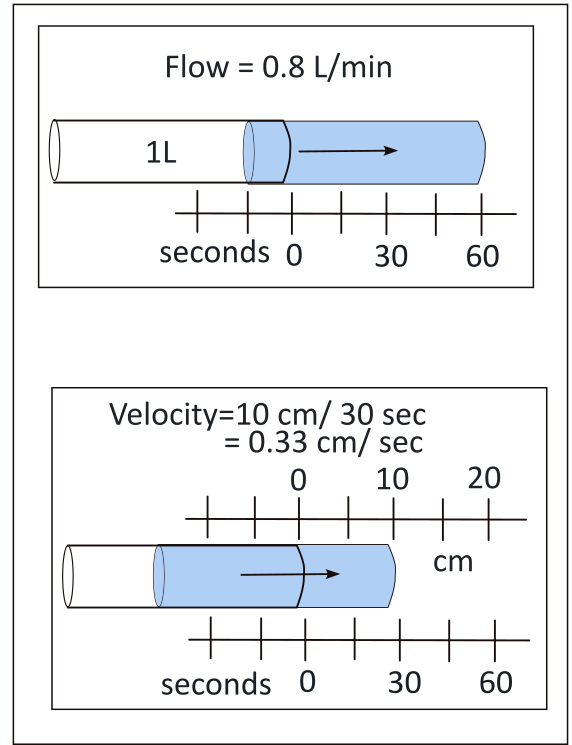
Flow is the volume (L) that moves in a unit of time (minute). Velocity is the distance (cm) moved in a unit of time (sec).
The top illustration shows a 1L volume moving to the right. In one minutes, 80% of it has moved. It is irrelevant how far it has moved; the point is 'what volume has moved in a minute'. This is flow.
By comparison, the lower illustration shows distance is being considered, not volume. After 'flowing' for 30 seconds it has only moved 10cm; how much was moving during that time is irrelevant. Simplfying, 10cm/30sec gives 0.33cm/sec. This is the velocity.
The Energy of Flow
Blood does not move because it is being squirted (ejected) from the heart! It moves because it is always moving, even just 'sitting there'. All matter, even blood, exhibits energy. It exists in two forms: the energy of motion (kinetic) and stored (potential) energy.
Kinetic Energy
All atomic particles are vibrating and rotating, larger particles such as atoms and molecules are moving in a line (translation), bouncing off each other and whatever object is in their path. The only way to eliminate all this motion is for it to reach a temperature of absolute zero...only theoretically possible.
Potential Energy
If the translational (forward moving) kinetic energy of a molecule runs into an 'immovable object', its forward motion becomes pressure. The energy still exists but is no longer expressed as motion...it is no longer 'kinetic'. Remove the 'immovable object' and off it goes again. That 'restrained' molecule had the 'potential' to move; it had potential energy.
Diastole
When the heart is in diastole (not contracting), oxygenated blood flows from the left atrium into the left ventricle, through the mitral valve. During this time the aortic valve 'exit' is closed. The cardiac muscles are relaxed and the compliant (stretchable) ventricle expands somewhat as it fills. No, it was not totally empty; it contained the 'non-ejected' blood (ESV) from the previous contraction. And the valve leading into the aorta is already closed, due to the potential energy against it at the aortic side.
When the pacemaker signals the myocardium (heart muscle) to contract, this external pressure on the contained blood increases its internal potential energy (PE). This pressure closes the mitral valve and prevents 'backflow'. The ventricle is now a sealed chamber and ventricular contraction continues.
Internally, the 'blood molecules' are still colliding against the ventricular wall...with ever increasing potential energy... that, when greater than that in the aorta, opens that valve. With an 'escape route', the potential energy converts to translational kinetic energy as blood is released into the aorta.
The Stroke
The aorta is not empty, it contains static, non-moving blood from the previous 'ejection'. Most of its initially 'forceful' energy was lost as 'work' by expanding the elastic aortic wall (dashed outline). In the center, kinetic energy continues 'translating' the blood downstream. With its departure, the elastic recoil (ER) of the aorta returns the vessel to a smaller diameter.
Velocity
Since blood is flowing, the potential energy exerted by 'wall-hugging' particles of stationary blood is now translational and 'dragging' against the vessel wall. The frictional resistance from this motion changes some of the energy to heat and the total energy of the blood is reduced. In large diameter vessels only a relatively small percentage of the blood is in direct contact with the vessel wall and the loss is minimal. In narrow vessels a relatively large percentage of the blood experiences wall-contact resulting in a significant energy drop.
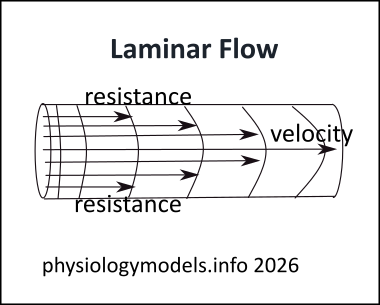
This resistance to flow reduces the velocity of the particles themselves. And these, in contact with 'more central' particles, reduces their velocity also, and so forth. The velocity of the most central particles have the greatest velocity. The illustration shows this laminar flow.
The explanation for this phenomonon is the relationship between resistance and vessel diameter. (The math calculations have been omitted to better concentrate on the concepts.)
Flow vs. Velocity
Tracking a small portion of blood through a straight series of vessels focuses on velocity...not flow. Velocity decreases throughout this path. Flow is when large volumes of blood are moving through the entire branching and recombining circulatory system. Flow is the same throughout this path.
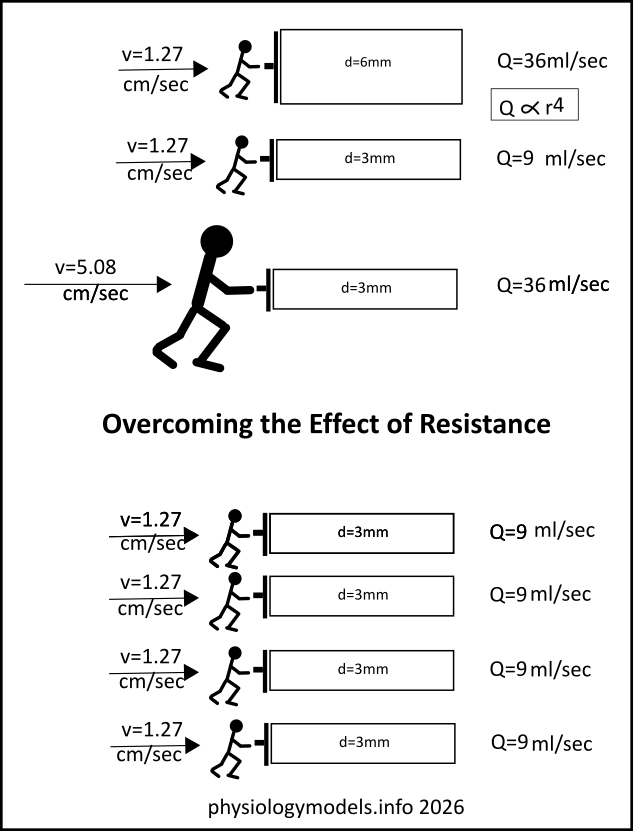
The top two images compare flow (Q) through a wide vs. a narrow tube...the diameter of the second is half that of the first.
The flow is not halved like the diameters are but is reduced exponentially by a factor of 4. To maintain this flow, the circulatory system uses four 3mm vessels to do the job. This is a major reason why capillaries are so numerous.
***************************
Heart
Cardiac Output
This illustration shows the minute volume (cardiac output (CO)) of blood leaving the left ventricle and the venous return (VR). The cardiac inhibitory and accelerator centers in the CNS determines the ventricular contraction rate and contractility. They receive input from the carotid sinuses (CS) and atrial stretch receptors (SR) resulting in reflexes that coordinate the inflow and outflow of ventricular blood.
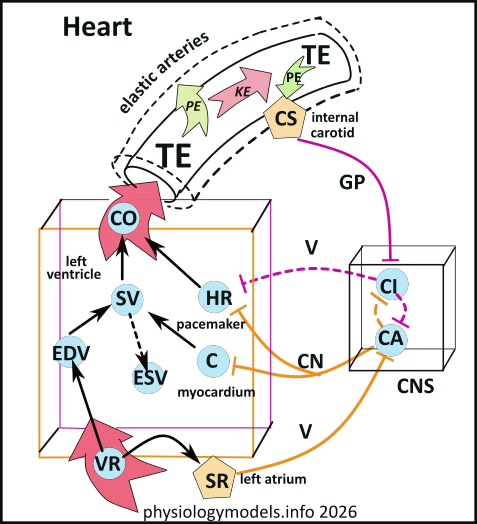
The blue circles represent important features involved in establishing blood flow. These are:
The two main factors that control cardiac output (CO) are stroke volume (SV) and heart rate (HR). The solid black arrows pointing from each of these toward cardiac output (CO) indicate that these are direct relationships; an increase in either stroke volume and/or heart rate will increase the cardiac output ... and vice versa.
Cardiac Output (CO)
The illustration shows two centers (CI & CA) in the central nervous system (CNS) reciprocally connected with dashed arrows...they inhibit each other. The 'inhibition' is not a 'stop' signal but rather a 'reduction' signal. When one center is strongly stimulated by an outside source it will reduce the activity of the other. After all, both centers target heart rate (HR) and stimulating and inhibiting it to the same extent would stop it!
The cardiac pacemaker (HR) has an intrinsic rhythm that can be modified by these centers. Both centers are active, to varying degrees, all the time. The cardioinhibitory center (CI) sends inhibitory signals (purple dashed line) to the pacemaker (HR) via the vagus nerve (V) and the cardioaccelerator center (CA) sends stimulatory signals (orange solid lines) to the pacemaker (HR) via the cardiac nerves (CN). The heart rate depends on which center is the most active.
Baroreceptor Reflex
As cardiac output increases, the pressure (PE) on the carotid sinuses (CS) also increases. Stimulatory signals (solid purple line) are sent, via the glossopharyngeal (GP) nerve, to the cardioinhibitory center (CI). From there, inhibitory signals (dashed lines) are sent to the pacemaker (HR) and the cardioaccelerator center (CA). The result is decreased heart rate .
The opposite is also true; a decreased CO will increase HR. These responses are called the Baroreceptor reflex. Its course is indicated by the purple lines in the illustration.
Venous Return (VR)
Bainbridge Reflex
Oxygenated blood from the lungs enters the left atrium. There are atrial stretch receptors (SR) near this entrance that send stimulatory signals (orange solid line), via the vagus nerve (V), to the CA center. This center has several outputs: inhibitory signals (dashed arrow) to the CI center to reduce its activity, and stimulatory (orange solid lines) signals, via cardiac nerves (CN), are sent to both the pacemaker (HR) and the heart muscle (myocardium) that increases its contractility (C). Contractility determines the force the ventricle exerts on the blood prior to its release into the aorta.
This is the Bainbridge reflex that 'responds' to venous return (VR) the same way the baroreceptor reflex 'responds' to the cardiac output (CO). Its course is indicated by the orange lines in the illustration. This pair of reflexes work to match the VR and CO so that the flow throughout the circulatory system is the same.
Stroke Volume (SV)
Venous Return (VR)
Starling's Law of the Heart states, "the more the heart muscle is stretched while it is filling, the more forcefully it will contract". This is an intrinsic behavior of cardiac muscle cells. How much the ventricle fills...stretching the cardiac muscle cells...depends on how long the heart remains in diastole (not contracting), before the next signal from the pacemaker, and how compliant (stretchable) it is.
While the heart is diastolic, venous blood is entering the ventricle and stretching it. The volume of blood, just before it contracts, is called the end diastolic volume (EDV). As the heart contracts (systole), most of this blood will be released; this amount is the stroke volume (SV) and that left behind is the end systolic volume (ESV). The greater the stretch the greater the contractility and the greater the contractility (C), the greater the stroke volume (solid arrow).
Contractility (C)
Typically 50-70% of the blood in the ventricle is released with each contraction...this is called the ejection fraction. The greater the SV the less the amount left behind (ESV)... an inverse relationship (dashed arrow). Blood is not actually 'ejected' in the sense that term is commonly used. The term 'released' is more appropriate based on current understanding of total energy as the 'force' involved in blood flow.
The contractility (C) or 'forcefulness' of systole depends on the intracellular concentration of calcium in myocardial cells. This is increased by stimulatory signals (orange solid line), via the cardiac nerves (CN), from the cardioacceleratory center (CA) This center's activity is increased by stimulatory signals (solid orange line) from the atrial stretch receptors (SR). These mechanoreceptors respond to atrial stretch due to the venous return (VR).
The combined effect of these two reflexes is that an increase in the venous return will result in an increase in the cardiac output. This seems rather obvious, at first glance, until realizing that contractility must be increased for this to be the case.
***************************
Arteries
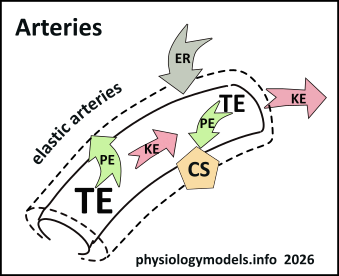
Flow used to be defined as movement along a blood pressure gradient but today it is defined as the movement along a total energy (TE) gradient. After all, 'blood pressure' is the measurement of potential energy at the inside of an artery at the peak of a pressure wave.
As blood moves downstream, losing energy in the process due to frictional resistance, it has less total energy than the blood from the next 'ejection'. The total energy gradient between the two exists because of the energy lost while the first was moving.
***************************
Arterioles
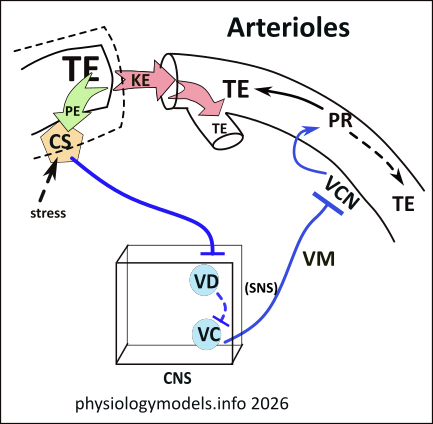
An arteriole is a branch off an artery that leads to a capillary bed. Their walls are mainly circular layers of smooth muscle. They are narrow, less than 1/10th of a millimeter, and energy drops quickly as blood moves within these 'resistance' vessels.
Vasomotor Reflex
Most arterioles are innervated by vasomotor nerves (VM), from the vasoconstrictor center (VC), that establishs a continuous baseline vasoconstriction (VCN). This is referred to as vasomotor tone. The diameter maintained allows sufficient flow to the tissues for everyday activities ('non-vital').
The vasomotor (VM) nerves responsible for this VCN belong to the sympathetic nervous system. They innervate arterioles leading to capillary beds of the digestive system, the kidneys, skin and mucous membranes and the bladder. Under stressful conditions, blood is shunted from these organs to 'vital' organs such as the heart and skeletal muscles.
Vasomotor tone is regulated by the carotid sinus (CS). There are a pair of these located where the common carotid arteries bifurcate into the internal and external carotids. The sinuses are at the start of the internal arteries. The sinuses activation 'set point' is a mean arterial pressure (MAP) of ~95mmHg. Note: MAP = systolic pressure + (2x diastolic pressure) / 3. At the 'set point', increasing blood pressure (PE) causes the carotid sinuses to stimulate (solid blue line) the vasodilator (VD) center, via the glossopharyngeal (GP) nerve. The VD center responds by inhibiting (dashed blue line) the ongoing activity of the vasoconstrictor (VC) center, thus increasing the dilation of the arterioles. This keeps the system-wide flow uniform.
Under heavy exercise or stressful conditions, flow to the above 'non-vital' tissues is reduces and that flow is diverted to the 'vital' brain and skeletal muscles. This occurs when the MAP reaches 120-150mmHg, the hypothalamus overrides the normal sinus behavior allowing the heart to race and vasoconstriction to redirect flow to the 'vital' organs, until the pressure drops. This is shown in the illustration by the 'backup' into a side branch.
***************************
Capillaries
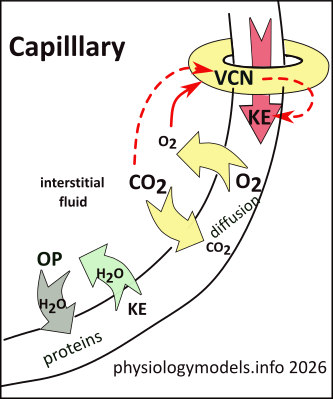
Capillaries have neither elastic fibers nor smooth muscle cells; they consist of a single layer of simple squamous endothelium. They are the sites of diffusion of respiratory gases--among other things--between the blood and interstitial fluid. Interstitial fluid in active tissues becomes oxygen poor and carbon dioxide rich; the reverse is true of inactive tissues.
Local Control
The entrance to a capillary bed is controlled by a smooth muscle precapillary sphincter that determines the size of the vessel opening. The extent of its vasoconstriction is not controlled by nerves but by the chemistry of the surrounding tissue. After all, the job of the blood is to transport respiratory gases, nutrients and wastes...inactive tissue do not require as much blood as do active ones.
The narrow capillaries require red blood cells move single file. And the resistance is so high that the velocity is very slow. This slow movement and closeness of particles to the capillary wall is key to the activities that occur in tissues.
Metabolically active tissues rapidly deplete the oxygen in the surrounding interstitial fluid and fill it with carbon dioxide. This low-oxygen environment establishes a concentration gradient for oxygen in the blood, to resupply the demand by diffusion. The same situation, in reverse, applies the the carbon dioxide waste product...it diffuses into the blood.
The low-oxygen environment has a direct relationship (solid arrow) with the vasoconstriction (VCN) of the sphincter...low oxygen causes low vasoconstriction. Additionally, the accompanying high-carbon dioxide environment is inversely related (dashed arrow) to vasoconstriction; high carbon dioxide causes low vasoconstriction. This pair of conditions opens the sphincter to allow good flow into the 'hungry' capillary bed.
Interstitial Fluid
In addition to delivering food and removing wastes from active tissues, capillaries are the source of the interstitial fluid. This is derived from the kinetic energy (KE)...most texts refer to it as hydrostatic pressure... of water molecules colliding with the thin capillary wall and passing through it. This occurs as long as the kinetic energy of the water molecules on the vessel's outer surface is less than the energy on the blood side.
Osmotic pressure (OP) is also a prime determinant of water balance. Particles, particularly proteins suspended in blood plasma, reduce the concentration of plasma's water molecules establishing a water gradient favoring the return of water to the plasma. An example of 'this gone wrong' occurs during starvation. The reduction of proteins reduces the osmotic pressure and the interstitial fluid increases. This is the cause of the bloated bellies of starving individuals.
***************************
Veins
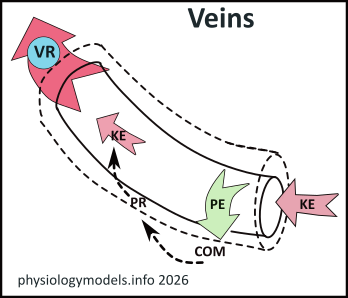
By the time blood leaves capillaries and enters the veins its total energy has been significantly reduced. The remaining translational kinetic energy (KE) is so low that the velocity has been reduced to a crawl.
Thankfully, the compliance (COM) ...stretchability...of veins is large enough to allow the remaining potential energy (PE) to maintain their expansion (dashed outline). This increase in diameter reduces the peripheral resistance (PR) (inverse relationship) to the extent that ~70% of the blood is in the veins. This large volume maintains the venous return (VR)...flow...but at a slow velocity.
There are several factors that assist this return:
***************************
...A Thousand Words
The job of the circulatory system is to supply food and oxygen to active tissues and remove waste and carbon dioxide. To achieve this, the vessels passing through the tissues must be numerous enough to be in close proximity to all the cells. They must be thin enough to allow for the passage of these substances through their walls. The velocity of blood passing through them must be slow enough for these things to occur.
From blood's exit from the left ventricle to the systemic capillaries, the vessels branch and rebranch multiple times. In the process, the resistance to flow increases exponentially, blood loses its energy, and slows progressively. Blood's return to the heart needs assistance supplied by valves in the veins, the thoracic pump, and vasoconstriction.
The blood's overall flow, through the various types of vessels, remains the same because of their branching and recombining, on the return trip to the heart. The return is 'sensed' by stretch receptors, that regulate the heart's contractility and rate, to pump this same volume out again. And, if it is pumped out too fast, pressure receptors near the outflow reduce the heart rate to slow it down.
The left ventricle supplies the energy for the blood to flow. By 'pressurising' this incompressible liquid, its potential energy increases to the point where it opens the aortic valve and escapes. The factors involved, leading up to this point, include the volume entering the ventricle, the contractility of the myocardium, and the heart rate...all intrinsically regulated.
The volume entering the ventrical depends on how long the myocardium is relaxed (diastole) and this depends on the heart rate. The heart rate and contractility applied to the upcoming stroke depends on the volume of blood that has entered. The greater this end diastolic volume, the greater the contractility and heart rate and the greater the volume 'ejected'... the stroke volume. Some blood remains in the ventricle, the end systolic volume, adding to the next inflow.
On exiting the ventricle, the blood's energy is sensed by the carotid sinuses that relay this information to the cardioinhibitory and vasodilator centers. The vasomotor reflex dilates arterioles leading to 'non-vital' organs and the heart rate is decreased. Together, these adjustments maintain system-wide flow. However, stressful conditions 'reset' the carotid sinuses to ignore these adjustments causing decreased flow to 'non-vital' organs and continued high heart rate. Blood is diverted to 'vital' organs during the stressful 'fight-or-flight' response.
At the capillary level, local chemical control increase flow into active tissues by sensing the blood gas concentrations in the interstitial fluid. The low-oxygen/high-carbon dioxide environment of these tissues causes the sphincter muscles at the entrance to this capillary bed to dilate. This supplies the needed oxygen and removes the waste carbon dioxide. The sphincter remains slightly constricted leading to inactive tissues.
The capillaries are the source of interstitial fluid within all tissues. Thin vessel walls allow water to be 'pushed' from the plasma into the surroundings; this push is routinely called 'hydrostatic pressure' but, in terms of the total energy of blood, 'kinetic energy' is more meaningful. Intersitital fluid is returned to the blood due to the 'pull' of plasma proteins referred to as 'osmotic pressure'.
After flowing through miles and miles of high-resistance capillaries, the total energy of the blood is very low. On entering compliant veins, the energy drop is even more pronounced. The resistance is low but so is the velocity of the blood and, to maintain system-wide flow, additional mechanisms assist. These consist of back-flow preventing valves, suction around the vena cavae during inhalation, and sympathetic stimulation of the veins.